Results speak
in millimetres
Selected case documentation — showing the protocol, the decisions, and the outcomes. Complex cases, long-term follow-up, and the invisible decisions that determine whether a result holds.
Complete digital workflow: photography protocol → DSD overlay → STL + DICOM integration → 6-implant guided surgery planning → scalloped bone reduction → immediate FP1 provisionalization. Soft tissue management integrated from the provisional phase — emergence profile conditioned over 5 months before final delivery.
Natural papilla formation. Optimal emergence profile. Stable peri-implant tissue architecture. Patient returned for contralateral arch — same protocol.
Combined guided bone regeneration and connective tissue grafting in a single surgical session — addressing hard and soft tissue deficiencies simultaneously. Non-resorbable membrane with titanium mesh, particulate xenograft, and subepithelial CTG for buccal mucosal augmentation. Tension-free primary closure.
Keratinised tissue augmentation stable. Bone volume confirmed on CBCT. Emergence profile indistinguishable from natural tooth. No recession at follow-up.
Two consultations. One surgery. Zero improvisation. Complete digital workflow from diagnosis to chairside — DSD, guided surgery with stackable guides, customised abutment for emergence profile development, and immediate temporisation. Simultaneous CTG for buccal mucosal augmentation.
Preserved interdental papilla. Natural emergence profile. No gingival recession at 24-month follow-up. Bone level stable on periapical radiograph.
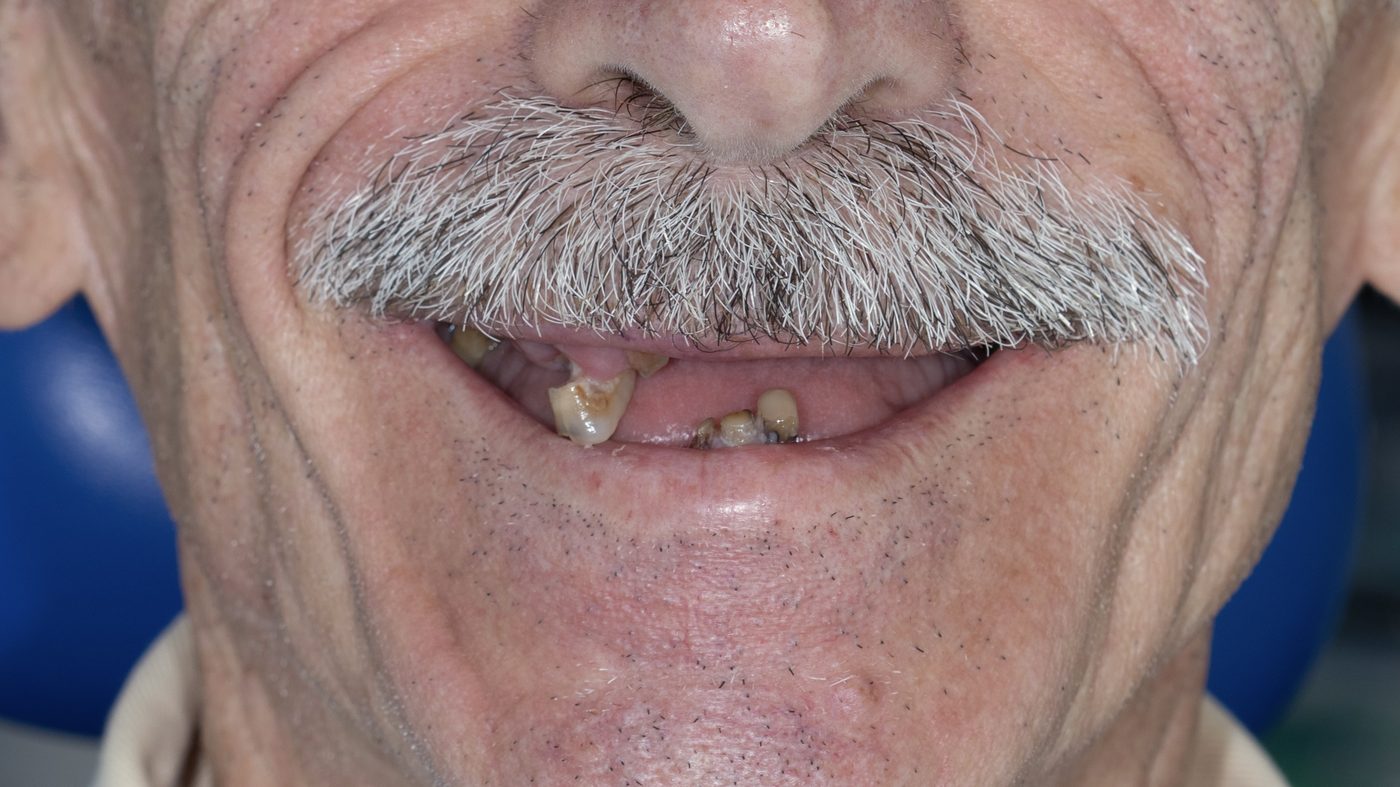

Full-arch rehabilitation of both the upper and lower jaw using the classic All-on-4 protocol — four implants per arch supporting an immediately loaded fixed prosthesis. The patient presented with severely compromised residual dentition, extensively fractured and decayed beyond restorative potential. Extractions, implant placement, and provisional prosthesis delivery were completed within the same surgical session.
Stable function and aesthetics maintained across both arches at three years. No prosthetic or implant complications recorded.


Root coverage of two Miller Class III (Cairo RT2) recessions — a 6mm recession at the mandibular left lateral incisor (tooth #32) and a 3mm recession at the maxillary right central incisor (tooth #11) — using a partly epithelialised connective tissue graft harvested from the maxillary tuberosity, placed via a tunnelling technique. Both sites were treated within the same surgical session, avoiding vertical releasing incisions and preserving papilla vascularity throughout.
Root coverage stable at seven years. Keratinized tissue width maintained. No further recession progression at either treated site.


Full-arch rehabilitation of the maxillary arch using the FP1 protocol — a tissue-level fixed prosthesis designed to replicate natural gingival architecture and tooth form. The residual dentition presented with extensive fracture and wear beyond restorative potential.
Provisional restoration, soft tissue handling, and final result
Natural-looking result maintained at three years, with harmonious integration between the prosthesis and surrounding soft tissue.


Aesthetic crown lengthening performed following orthodontic treatment to correct gingival display and even out clinical crown height across the anterior sextant, combined with vital tooth whitening to complete the aesthetic result.
Balanced gingival architecture and improved tooth proportion maintained at follow-up, with a brighter, more uniform shade across the smile.